WHEN IS SYMMETRICAL NOT SYMMETRICAL?
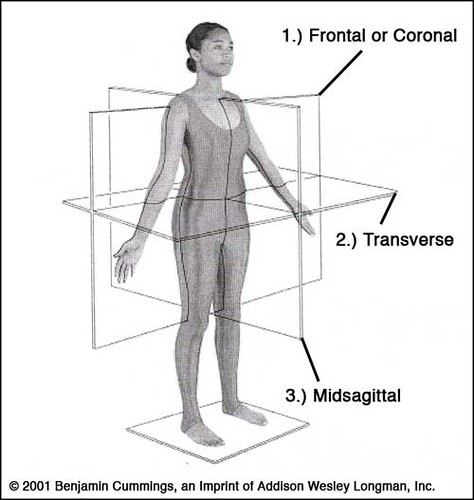
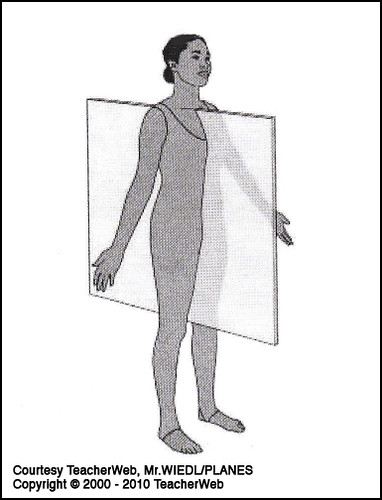
The first installment of this series discussed the anatomical position and planes. The focus was on the midsagittal plane, which is a theoretical construct dividing the body into symmetrical right and left halves. The right and left sides of the body are supposed to be mirror images of each other in length, girth, and muscle power.
It is important to establish baseline measurements of each respective side of the body. This will assist the coach in determining the individual's current physical status. If the athlete has equal strength in all muscle tests on each side of the body, the coach can then direct the athlete to a progressive training program. If the athlete exhibits inequalities between the two sides, then she must be directed to a corrective exercise program. Many athletes will have ipsilateral (same side) upper and lower extremity dominance. Some will have contralateral (opposite side) upper and lower extremity dominance. Some will be ambidextrous.
Regardless of one's respective upper and lower body dominance, it is important in weightlifting to have both sides of the upper extremities, lower extremities, and torso equal in strength and alignment. The first part of this series made reference to establishing a baseline of strength in the beginning female weightlifter. In this installment, the following measurements and functional testing procedures will be discussed:
1.) Circumferential Measurements
2.) Leg Length & Asymmetry
3.) Spinal Alignment
4.) Muscle Testing
1. CIRCUMFERENTIAL MEASUREMENTS
More often than not the athlete's dominant side is larger in girth and stronger than the non-dominant side. Muscle size does not necessarily represent the muscle's force output, but it is always important to develop parity in size between the right and left sides of the body.
For the upper body circumferential measurements should be taken on both sides of the body for the following parts:
-Upper arm
-Forearm
-Wrist
-Hand
For the lower body, circumferential measurements should be taken on both sides for the following parts:
-Thigh
-Lower leg
2. LEG LENGTH & ASYMMETRY
It is important to have equal leg length. Unequal leg length or leg length discrepancy can affect the rest of the body; it can disturb position of the foot stance, squatting position, pelvic stability, and the entire spinal alignment.
When considering leg length, one must measure from the anterior superior iliac spine (ASIS) of the pelvis to the inside bone of the ankle, the medial malleolus (Fig. 1).
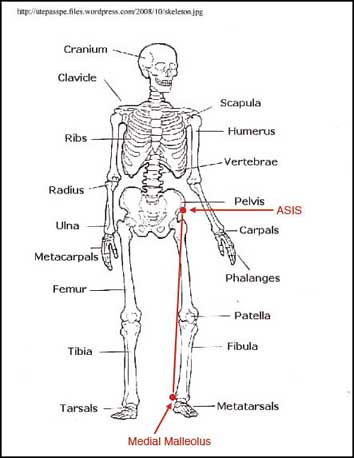
Figure 1: Leg Measurement Points
If there is a question of leg length discrepancy, then the athlete should be referred to an appropriate healthcare professional who can evaluate it further.
3. SPINAL ALIGNMENT
As part of the evaluative process, the beginning lifter should be tested for scoliosis. The word scoliosis comes from the Greek skoliosis meaning "crooked." It is not uncommon for females between the age of 10-16 to have idiopathic "unknown origin" scoliosis.
A basic test to detect spinal alignment issues is the Adam's Test (Fig.2). In this test, the lifter is required to wear the appropriate clothing to allow proper observation. The athletes will be requested to bend forward and allow their upper spine to round with their arms dangling. The legs are kept straight and the feet are equal in their stance.

Figure 2: Adam's Test
Source: iscoliosis.com
The examiner should observe from both the front and back of the bent-over athlete. If the examiner observes a deviation from a straight spinal alignment or some form of rotation ("increased height") on one side of the spine, then the individual should be recommended to the appropriate health practitioner.
4. MUSCLE TESTING
Shoulder Abduction. The motion of shoulder abduction is controlled by the deltoid muscle. The deltoid muscle is in turn neurologically controlled by the C5 nerve root. The deltoid muscle (as seen in Fig. 3) controls lifting the arm out to the side of the body. It is also very valuable in contributing to overhead movement. The athlete is tested by holding their arm out to the side (abducting) with their thumb pointing down against resistance in the downward motion. lf the athlete cannot tolerate minimal resistance, the downward direction then specific exercises should be prescribed to strengthen the deltoid muscle.

Figure 3: Shoulder Abduction
Shoulder internal rotation/external rotation (Fig. 4, Fig. 5) are tested for the main reason that in the female weightlifter, the rotator cuff muscles of the shoulder are important stabilizers of the shoulder joint. Stabilizing the shoulder joint is important to diminish the chances of shoulder dislocations in the beginning female weightlifter.

Figure 4: Internal Rotation of the Shoulder

Figure 5: External Rotation of the Shoulder
Elbow Flexion. The motion of elbow flexion is controlled by the biceps muscle. The biceps muscle is neurologically controlled by the C6 nerve root. When testing the power of the biceps muscle the examiner will place resistance on the inside of the hand or wrist of the athlete while the athlete prevents the examiner from straightening the elbow (Fig. 6).

Figure 6: Elbow Flexion
Elbow Extension. The motion of elbow extension is controlled by the triceps muscle. The triceps muscle is neurologically controlled by the C7 nerve root. When testing the power of the triceps muscle the examiner will place resistance on the outside of the hand or wrist of the athlete while the athlete prevents the examiner from bending the elbow (Fig. 7).

Figure 7: Elbow Extension
Elbow flexion and elbow extension are important to maintain the integrity of the elbow joint. There is always the concern of elbow dislocations in beginning female weightliiters, so corrective exercises should be prescribed at the beginning of a female weightlifter's career.
Finger Abduction. The motion of finger abduction is controlled by the finger abductors. The finger abductors on neurologically controlled by the C8 nerve root. When testing the power of the finger abductors, the athlete will try to hold the fingers apart while the examiner tries to close them (Fig. 8).
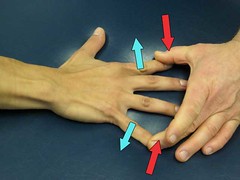
Figure 8: Finger Abduction
Finger Opposition. The motion of finger opposition occurs when the thumb and pinky are held together (Fig. 9). The examiner tries to pull the thumb and pinky apart. Finger opposition is neurologically controlled by the T-1 nerve root.
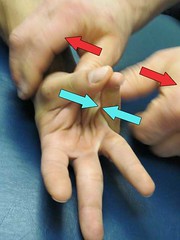
Figure 9: Finger Opposition
Finger motions are important in the beginning female weightlifter to maintain a secure grip on the bar.
Hip Abduction. Abduction of the hip occurs when the leg is moved away from the midline of the body. Abduction is neurologically controlled by the L3 L4 and L5 nerve roots. If the athlete is asked to abduct the leg whether in a supine or sideline and cannot maintain a nominal resistance against the examiner then corrective exercises should be initiated (Fig. 10). Weakness in the hip abductor muscles will cause beginning, intermediate, and advanced female athletes to have "kissing knee syndrome." Kissing knee syndrome is a very common problem in female weightlifters. When females squat or recover from the squat clean, the knees may come together. This knee-together pattern will cause excessive stress on the medial (middle) tissues of the knee. The motion is also biomechanically less effective than maintaining hip abduction and keeping the knees apart.

Figure 10: Hip Abduction
Hip Extension. Extension of the hip is tested when the athlete is laying prone on a surface and lists their leg toward the ceiling (Fig. 11). The examiner attempts to resist the upward motion of the lower extremity. Weakness in hip extension represents problems with the gluteal and hamstring musculature. This musculature will strengthen as the beginning female weightlifter matures, but corrective exercises can be prescribed to strengthen the muscles faster.

Figure 11: Hip Extension
Knee Extension. Extension of the knee is tested with the athlete sitting upright on a stable surface with the knee at the edge of the surface, so that the lower leg is hanging freely. The examiner requests the athlete to extend the lower leg and provides resistance to the front of the lower shin (Fig. 12). Knee extension is controlled by the quadriceps muscles and is neurologically mediated through the L2-L3-L4 nerve roots.

Figure 12: Knee Extension
In the next installment of this series, we will discuss and demonstrate various exercises you can use to test the strength and balance of the upper body, lower body, and trunk.
Copyright © 2010 Marc Chasnov